
Complex PTSD symptoms have been the hardest in psychotherapy to treat. Trauma that comes from repeated, prolonged exposure, which is most often rooted in Adverse Childhood Experiences (ACEs), doesn’t respond the same way as single-event PTSD. Clients struggle through standard exposure protocols. Many drop out. Many improve, then relapse. Many never get diagnosed correctly in the first place.
In India, the problem is sharper. Most trauma research has been conducted on Western populations and Western-style trauma — single events, military combat, and accidents. The childhood trauma our clients carry — joint-family dynamics, comparisons that taught them they were never enough, abuse hidden under the language of discipline — has rarely been the subject of published research.
In 2024, we set out to change that.
What we tested
Our team at Wellness Space ran a quasi-experimental pilot study, published in the European Journal of Trauma & Dissociation, that asked a single, specific question: could Reconsolidation of Traumatic Memories (RTM), a protocol that uses memory reconsolidation through dissociated recall, meaningfully reduce CPTSD symptoms in adults living with childhood trauma in India?
Evidence-based psychotherapy approach using RTM for PTSD and CPTSD
We used the International Trauma Questionnaire (ITQ) to measure CPTSD severity. We tracked scores at baseline, at one month after intervention, and again at three months. We also identified index-trauma events and addressed trauma footprint of those events.
The cohort was urban Indian adults presenting with CPTSD symptoms — anxiety, hypervigilance, intrusive memories, difficulty regulating emotions, and persistent low self-worth. Many had tried other forms of therapy. Most had multiple Adverse Childhood Experiences on the Trivedi ACE-14 Assessment, our India-specific assessment tool.
What we found
The paired t-test showed a statistically significant reduction in CPTSD scores at both the one-month and three-month marks (p<.01). Not just an immediate improvement that faded, but a sustained reduction across three months.
Three things stood out to us clinically:
The drop-out rate was lower than what’s typically reported for Trauma-Focused CBT. This matters. CPTSD clients often cannot tolerate exposure-based approaches. They dissociate, shut down, or simply stop coming back. RTM’s dissociated-recall protocol, what we call the “movie theatre” technique, gives the client distance from the memory while it is being updated. They don’t have to retell the story in detail. They don’t have to feel it again.
Symptoms shifted across categories, not just one. Reductions were observed in re-experiencing, avoidance, and disturbance in self-organisation, which constitute the three core CPTSD clusters.
Combining RTM with inner child therapy seemed to support the deeper work. Several cases benefited from inner-child work in the early sessions, before the index memory was addressed with RTM. This pattern of safety first, memory second, was something we’d been observing clinically. The pilot data were consistent with it.
Why this matters in India
CPTSD is widely under-recognised here. Standard psychiatric assessments in India still default to PTSD or depression even when the client’s history shows years of repeated childhood adversity. ICD-11 added CPTSD as a distinct diagnosis in 2022. But translation into Indian clinical practice has been slow.
Our published findings, alongside two further Cureus case studies: Trivedi (2024) (a single-case study using RTM for CPTSD) and Shetty, Trivedi & Bhatia (2026) (trauma-informed psychotherapy for CPTSD in a young adult woman), make a clinical case for offering RTM as a primary option, not just a fallback, for clients with CPTSD rooted in childhood.
Where does this fit at Wellness Space?
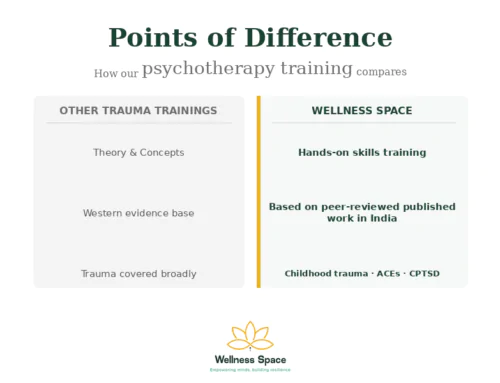
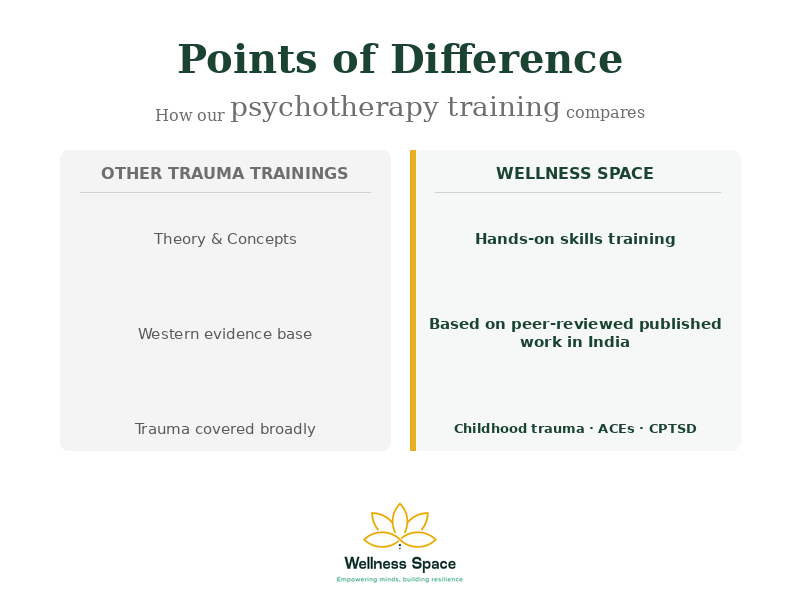
RTM is taught in clinical detail in Module 4 of our evidence-based psychotherapy training and reinforced across the advanced trauma-informed psychotherapy modules. Our training is the only EARTh-, IMDHA-, and IPHM-accredited evidence-based psychotherapy programme in India that includes RTM as a core protocol.
For therapists, the question of whether RTM “works” is no longer theoretical. The evidence base is real and growing. The question now is whether your clients with CPTSD have access to it.
For individuals, if you’ve tried therapy that hasn’t moved your CPTSD symptoms, or if you’ve been told to “talk it through” with a memory you cannot bear to revisit, there is another way.
A complete guide to RTM in India, including the comparison with EMDR and CBT, the neuroscience of memory reconsolidation, and step-by-step session structure, is on our RTM pillar page.
References
Trivedi, G. Y., Pandya, N., Thakore, P., Ramani, H., Trivedi, R. G., & Kathirvel, S. (2024). The effectiveness of Reconsolidation of Traumatic Memories for Complex PTSD – A pilot quasi-experimental study from a wellness centre in India. European Journal of Trauma & Dissociation, 8(4), 100480. https://doi.org/10.1016/j.ejtd.2024.100480
Shetty, Y. N., Trivedi, G. Y., & Bhatia, G. (2026). Trauma-Informed Psychotherapy for Complex Post-traumatic Stress Disorder in a Young Adult Woman: A Case Report. Cureus, 18(3), e105984. https://doi.org/10.7759/cureus.105984
Trivedi G. Y. (2024). Reconsolidation of Traumatic Memories in the Treatment of Complex Post-traumatic Stress Disorder (CPTSD): A Case Study. Cureus, 16(9), e68927. https://doi.org/10.7759/cureus.68927
Related reading at Wellness Space

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Leave A Comment