
Introduction
Many adults spend years struggling with anxiety, depression, burnout, relationship difficulties, low self-worth, perfectionism, or emotional overwhelm without fully understanding where these challenges began. Increasingly, research suggests that the roots of many adult difficulties may lie in childhood experiences.
In psychotherapy, these experiences are often described as childhood trauma or inner child wounds. In public health research, they are referred to as Adverse Childhood Experiences (ACEs). Although the terminology differs, both concepts highlight the lasting impact that childhood experiences can have on emotional, psychological, social, and physical well-being.
Both terms (childhood trauma or ACEs) broadly point to the same territory. But the picture is incomplete without its other half: Positive Childhood Experiences, or PCEs — the protective experiences that, our latest research now shows, independently shape adult resilience.
Until recently, this entire research in the area of childhood experiences has been mapped almost entirely from outside India, using Western populations, Western family structures, and Western definitions of what constitutes adversity. Over the past 8 years, we at Wellness Space have been building the Indian map. This post explores what research has taught us about childhood trauma, how it can affect adults later in life, how parents can help break the cycle, and what we now know about healing and resilience through PCEs.
Childhood trauma, ACEs, and PCEs — defined
Childhood trauma is the everyday term for the impact of adverse events that happened before age 18. Adverse Childhood Experiences (ACEs) is the framework researchers use to measure those events systematically. Positive Childhood Experiences (PCEs) is the framework researchers use to measure the protective experiences that run alongside them — supportive caregivers, a sense of belonging, predictability, at least one trusted adult.
The ACE framework began in 1998 with the original Kaiser-CDC study in the United States (Felitti et al., 1998), which identified ten categories of childhood adversity across three groups:
- Abuse — physical, emotional, or sexual
- Neglect — physical or emotional
- Household dysfunction — parental separation, parental mental illness, parental substance abuse, parental incarceration, witnessing domestic violence
The original study established something the trauma field had long suspected but had never measured at scale: the more ACEs a person reports, the higher their risk of adult anxiety, depression, cardiovascular disease, diabetes, and shortened life expectancy. This is what is meant by a dose-response relationship; anincrease in dosage, or each additional ACE, adds measurable incremental risk.
PCEs entered the research conversation more recently, especially in India. They are not simply the absence of ACEs. They are independently protective, meaning two adults with the same ACE load can have meaningfully different outcomes depending on what positive experiences ran alongside the adversity. This insight is what makes recovery work possible at all.
The dose-response finding matters because it tells you childhood trauma is not all-or-nothing. The question is not whether your childhood was “traumatic enough” to count. The question is how much adversity was carried, what protective experiences ran alongside it, and how both show up now.
The table below summarises the three concepts at a glance:
| Aspect | Childhood Trauma | Adverse Childhood Experiences (ACEs) | Positive Childhood Experiences (PCEs) |
| What it is | Psychological and developmental impact of childhood experiences | Framework for measuring childhood adversity | Framework for measuring positive and protective childhood experiences |
| Primary question | How did these experiences affect me? | What adverse experiences happened? | What positive experiences supported me? |
| Focus | Emotional, psychological, and developmental consequences | Exposure to adversity | Exposure to safety, support, connection, and belonging |
| Origin | Clinical psychology and psychotherapy | Public health and epidemiological research | Resilience and developmental research |
| Perspective | Individual experience and meaning | Risk factors | Protective factors |
| Examples | Emotional neglect, abuse, bullying, humiliation, rejection, chronic criticism, and emotional invalidation | Three clusters: Abuse (physical, emotional, sexual), Neglect (physical, emotional), and Household Dysfunction (e.g., parental separation, domestic violence, substance misuse, mental illness in the household) | Feeling loved, having trusted adults, a sense of belonging, supportive friendships, feeling safe and valued |
| Measures impact? | Yes | No, primarily measures exposure | No, primarily measures exposure |
| Role in mental health | Helps explain symptoms, emotional difficulties, and behavioural patterns | Helps identify risk for future mental and physical health problems | Helps identify resilience and protective influences |
| Used in therapy? | Frequently explored in psychotherapy and trauma-informed care | Routinely used as a structured assessment or screening tool to understand childhood adversity and risk factors | Increasingly used to identify strengths, protective factors, and sources of resilience |
| Focus on risk or protection? | Primarily, the consequences of adversity | Risk factors | Protective factors |
| Influences adult relationships? | Yes | Yes | Yes |
| Influences parenting? | Yes | Yes | Yes |
| Can it be changed later? | The experiences cannot be changed, but their effects can be understood, healed, and integrated | Past exposures cannot be changed, but their impact can be reduced through healing, support, and resilience-building | Similar protective experiences can be developed and strengthened throughout adulthood |
| Key message | Understanding wounds and their effects | Understanding adversity and risk | Understanding strengths and resilience |
A simple way to think about these concepts is this: ACEs help us understand what went wrong, PCEs help us understand what went right, and childhood trauma helps us understand how those experiences shaped us. Together, they provide a more complete picture of risk, resilience, recovery, and mental well-being.
Why India needed its own research on childhood experiences
Two problems with applying the original ACE framework to Indian adults.
First, the original ACE-10 questionnaire was designed for American family structures. It does not capture forms of childhood adversity that are common in Indian households; joint-family dynamics where authority is diffused across multiple adults, comparison-based shaming as a parenting style, the conflation of “discipline” with physical or emotional abuse, and the heavy weight placed on academic achievement and social conformity. An Indian adult can score zero on ACE-10 and still carry significant childhood trauma.
Second, the published evidence base on what ACEs and PCEs do in Indian populations was almost non-existent until recently. Treatment recommendations for childhood trauma in India were being drawn from research done on populations very different from the people sitting across from Indian therapists.
Both gaps drove the work we have been doing.
Indian research finding 1 — the ACE dose-response holds here too
In a cross-sectional study of 909 adults at Wellness Space, published in 2025 in the Indian Journal of Community Medicine, our team examined the relationship between ACE exposure and adult mental health in an Indian clinical population. The finding was clear: the same dose-response relationship documented in Western research holds in Indian adults. The more ACEs reported, the higher the adult anxiety and depression scores.
This may sound expected. It is not. Research questions in psychology do not translate automatically across cultures, and one genuine risk in evidence-based practice is assuming they do. The 909-person finding suggests that the ACE framework is highly relevant for understanding how childhood adversity translates into adult mental health difficulties in Indian clinical populations.
The earlier 2021 paper by Dr Gunjan Y Trivedi, published in the Journal of Preventive Medicine and Hygiene, made the public-health case for why this matters: India urgently needs preventive and clinical intervention around ACEs, not just downstream treatment of the adult conditions they cause.
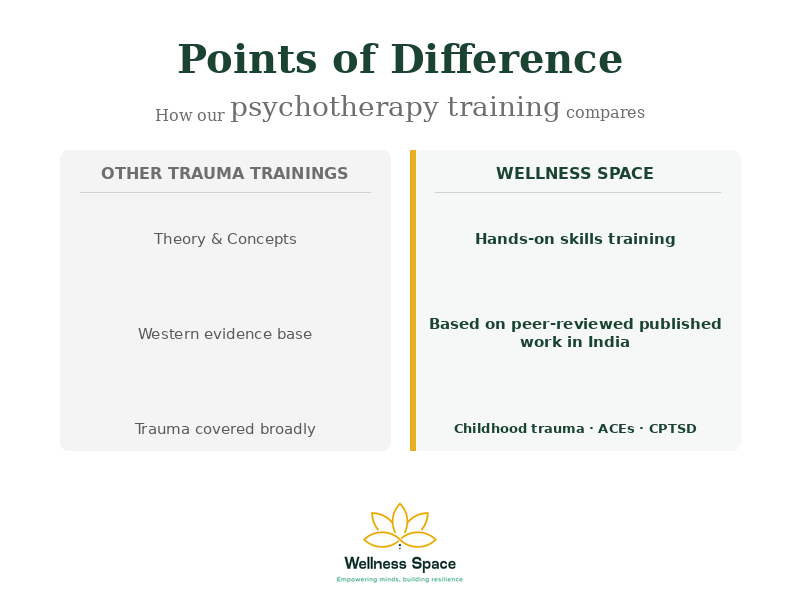
Indian research finding 2 — the Trivedi ACE-14 Assessment™
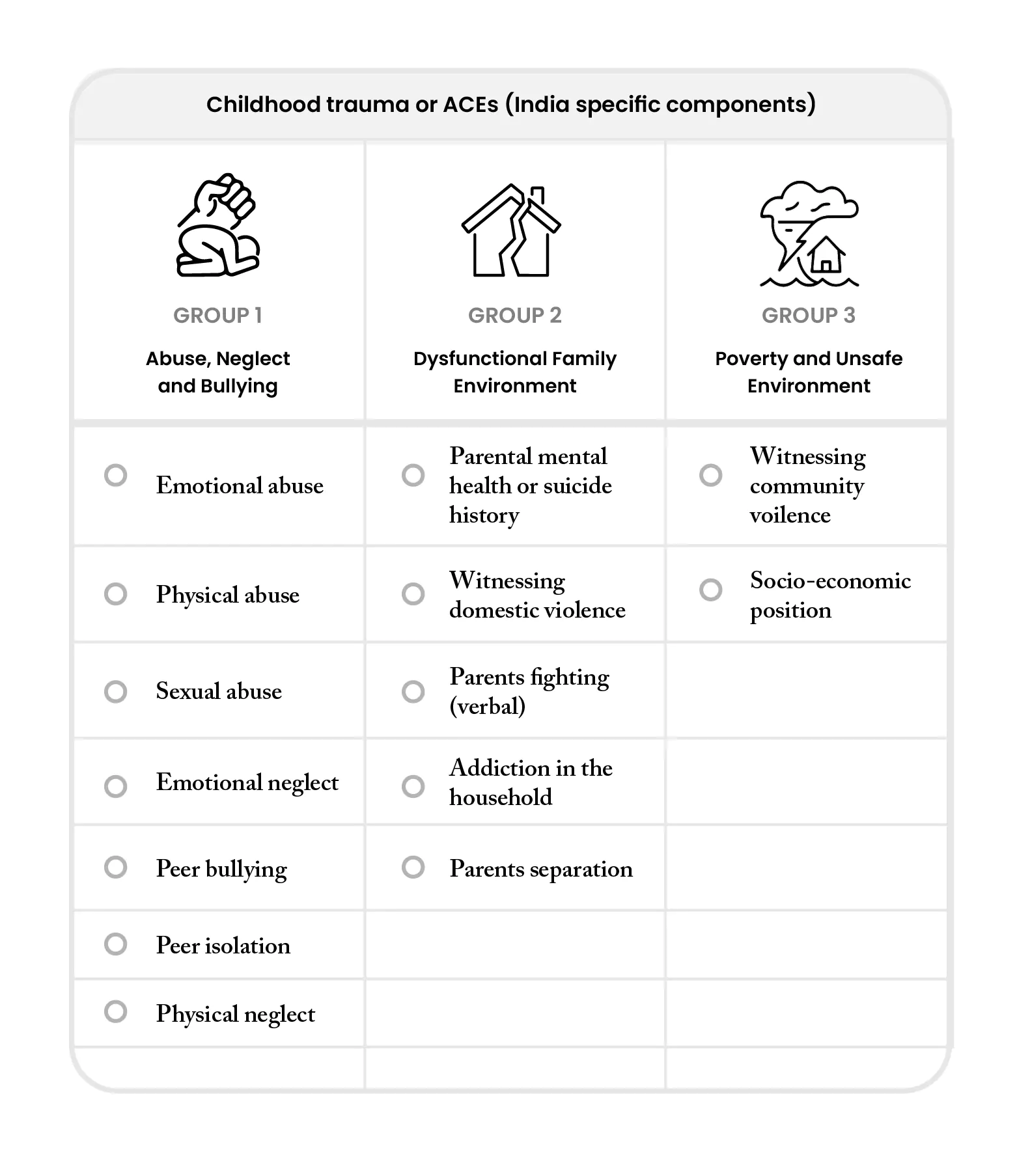
Building on the gaps in the original ACE-10 for Indian contexts, our team developed the Trivedi ACE-14 Assessment™. It revises the original ten ACE items and adds four India-specific items capturing forms of childhood adversity that the original instrument misses. These additional items were derived from clinical observation across thousands of Indian client sessions and validated through subsequent research. (Visual from our book covering all the key PCEs is shown here. The details of the book are at the end of the article)
The practical implication: an Indian adult who scored low on ACE-10, and was therefore told their childhood was not a clinical concern, may score significantly higher on ACE-14, with their actual experiences now visible. This changes assessment, formulation, and the choice of therapeutic approach.
The Trivedi ACE-14 Assessment™ is used in every intake at Wellness Space and is the assessment instrument our team uses in our published research. While ACE-14 helps identify adversity that may otherwise remain hidden, PCE research reminds us that resilience is shaped not only by what went wrong, but also by what went right.
Indian research finding 3 — Positive Childhood Experiences also count
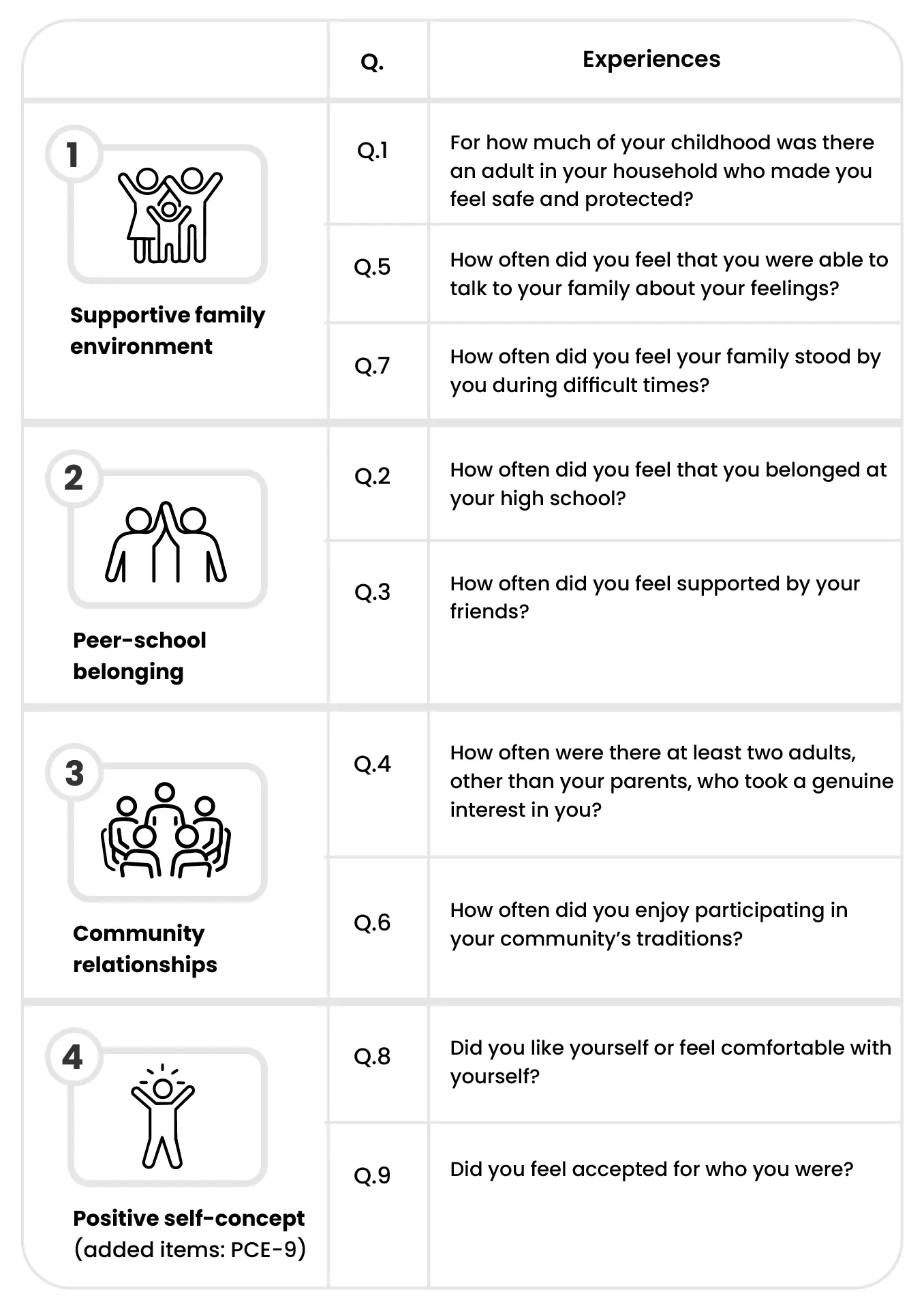
The picture would be incomplete if we stopped at adversity. In 2026, Dr Gunjan Y Trivedi published a paper in Acta Psychologica asking a different question: do Positive Childhood Experiences (PCEs) also leave a measurable mark on adult outcomes in Indian populations? (Visual from our book covering all 14 ACEs is shown here. The details of the book are at the end of the article).
The finding: yes. Positive childhood experiences i.e., supportive caregivers, at least one trusted adult, a sense of belonging, predictability, are independently associated with adult resilience, even after accounting for ACE exposure. People with high ACE scores who also report high PCE scores do better on adult mental health outcomes than people with the same ACE load but fewer protective experiences.
Two things make this finding clinically important. First, PCEs are independently protective — they are not simply the inverse of ACEs, and an adult does not need a zero ACE score to benefit from a high PCE score. Second, the same finding holds in an Indian sample, which means clinical and preventive recommendations grounded in PCE research are now justified for Indian populations, not just imported on faith from Western data.
In plain language: childhood trauma is not destiny. The protective experiences that ran alongside it, even small ones, like one steady adult, one safe friendship, one place that felt predictable — also shaped you. And the protective experiences an adult builds now, in therapy, in relationships, in rebuilding routines that provide safety, continue to shape outcomes well beyond childhood.
Even within the same family, siblings may have different outcomes because they experience different combinations of adversity, protection, temperament, relationships, and life circumstances.
How childhood trauma shows up in adult life
Across the 20,000+ hours of clinical work our team has logged at Wellness Space, certain patterns appear consistently in adults carrying a significant ACE load:
- Chronic anxiety that persists despite lifestyle changes, self-help efforts, or the absence of obvious current stressors.
- Persistent low self-worth that survives professional success and external validation
- Difficulty regulating intense emotions — disproportionate anger, shutdown, or numbing
- Sleep disturbance and somatic symptoms (chronic gut issues, headaches, unexplained chronic pain) that have been medically worked up and not resolved
- Relationship patterns that repeat — choosing partners who replicate the family-of-origin dynamic, or being unable to ask for need-meeting
- A subtle sense that something is wrong with you, despite all evidence to the contrary
These are not personality flaws. They are, in our clinical view, the adaptive responses a child developed to survive a particular family environment, now showing up in an adult life where they are no longer adaptive. The fact that they were once protective is part of what makes them hard to change.
Complex PTSD (CPTSD): when childhood trauma was prolonged
Not all childhood trauma results from a single event. For many people, adversity occurs repeatedly over months or years through emotional neglect, chronic criticism, abuse, bullying, family conflict, or other ongoing experiences. In such cases, the clinical picture may be better understood as Complex Post-Traumatic Stress Disorder (CPTSD).
CPTSD was formally included in the ICD-11 diagnostic system in 2022. In addition to the three core PTSD symptoms; re-experiencing, avoidance, and a persistent sense of threat, it includes a broader pattern known as Disturbances in Self-Organisation (DSO). These difficulties may appear as emotional dysregulation, a persistently negative view of oneself, shame, low self-worth, and ongoing problems in relationships.
Importantly, CPTSD appears to be far from rare. A major review published in The Lancet Psychiatry reported that approximately half of individuals seeking treatment in mental health services may meet criteria for CPTSD rather than PTSD alone, highlighting the significant role of prolonged and repeated trauma in clinical populations.
In India, individuals with histories of prolonged childhood adversity may still be diagnosed primarily with anxiety, depression, or PTSD, even when their experiences and symptoms are more consistent with CPTSD. Recognising this distinction is important because prolonged developmental trauma often requires approaches that address emotional regulation, self-concept, relationships, and unresolved childhood experiences, not only trauma memories themselves.
At Wellness Space, treatment for childhood trauma is informed by both trauma-focused and developmental approaches. One of our published studies found that Reconsolidation of Traumatic Memories (RTM), a brief trauma-processing protocol, was associated with significant reductions in CPTSD symptoms among Indian adults at one- and three-month follow-up assessments (Trivedi et al., 2024). RTM is often used alongside Inner Child Therapy and other trauma-informed approaches to support recovery from the long-term effects of childhood adversity.
At Wellness Space, Inner Child Therapy and RTM serve complementary roles. Inner Child Therapy helps individuals understand and work with the developmental origins of emotional patterns, while RTM focuses on reducing the emotional intensity of unresolved traumatic memories. Together, these approaches form part of our broader evidence-based psychotherapy framework for childhood trauma and CPTSD.
The growing recognition of CPTSD symptoms in individuals arriving at mental health centers reinforces an important message: many adults who struggle with chronic shame, emotional overwhelm, relationship difficulties, or a persistent sense of “something being wrong with me” may actually be living with the lasting effects of prolonged childhood trauma, and effective help is available.
What the recovery path looks like
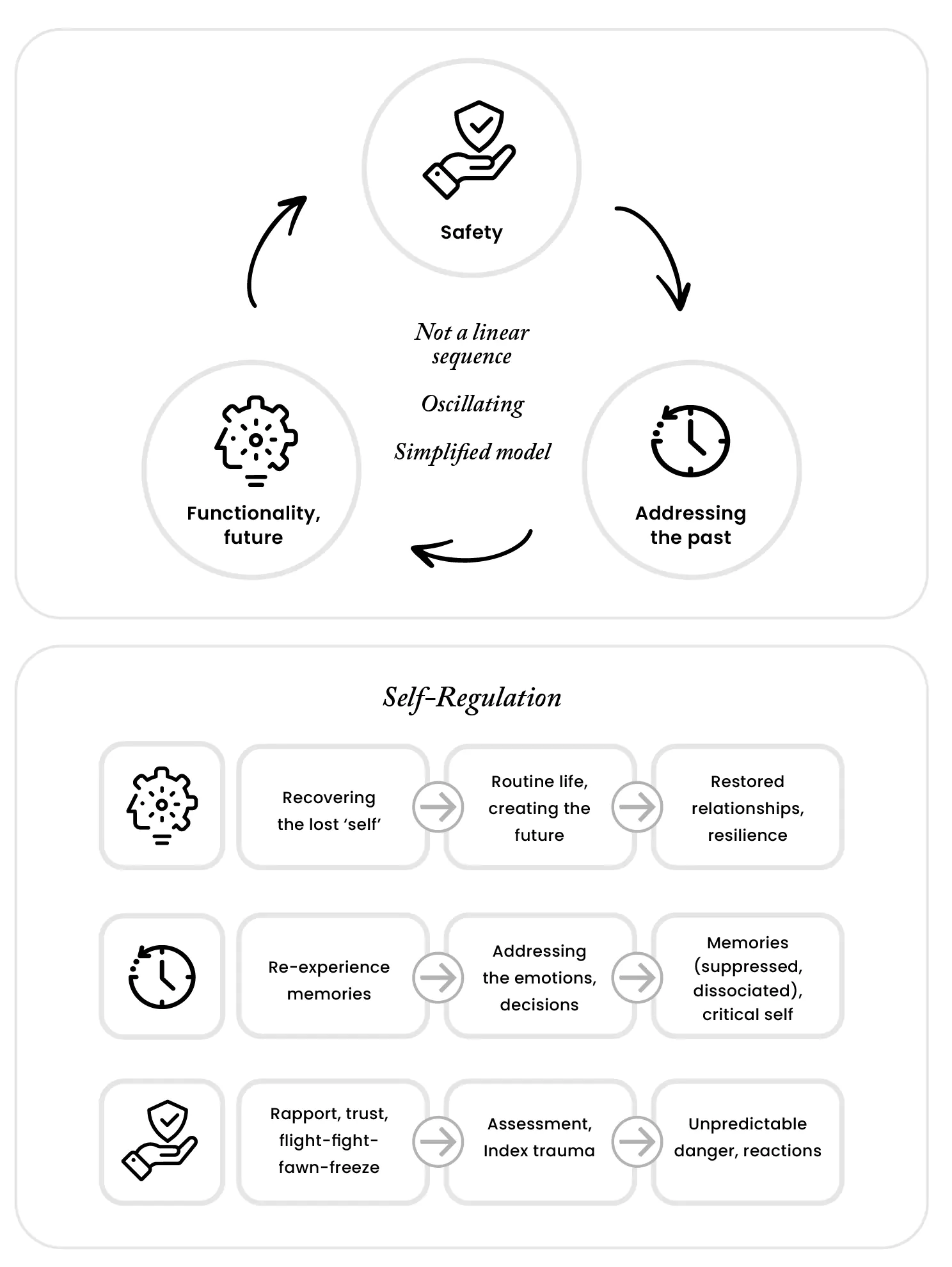
Recovery from childhood trauma is rarely a straight line (Visual from our book showing the recovery model from childhood trauma is shown here. The details of the book are at the end of the article). At Wellness Space, we view recovery as a dynamic process that involves three interconnected tasks: creating safety in the present, addressing unresolved experiences from the past, and rebuilding a meaningful future through resilience, relationships, and everyday functioning. People often move between these areas repeatedly as new insights emerge and old patterns begin to change.
The full framework, along with practical exercises, clinical examples, and evidence-based approaches to recovery, is explored in What Happened to Me? vs What’s Wrong with Me?: Indian Perspectives on Childhood Trauma and Recovery. For readers seeking a deeper understanding of childhood trauma and a roadmap for healing, the book provides an accessible and comprehensive guide grounded in both research and therapeutic practice.
Recovery is most effective when it is guided by evidence-based psychotherapy. Evidence-based psychotherapy refers to therapeutic approaches that are informed by scientific research, clinical expertise, and the needs of the individual. In the context of childhood trauma, this may include trauma-informed psychotherapy, Inner Child Therapy, attachment-informed approaches, self-regulation interventions, and trauma-processing methods such as Reconsolidation of Traumatic Memories (RTM). Different approaches may be appropriate for different individuals depending on their history, symptoms, strengths, and goals.
The intergenerational link — what this means for parenting
If you are a parent reading this, there is a part of the story we cannot leave out. Childhood trauma is intergenerational by default. The unhealed adversity an adult carries shapes how they parent, not because they intend it to, but because regulation, attachment, and the capacity to be emotionally available to a child are all affected by what that adult’s own childhood looked like. ACE research consistently shows this transmission pattern: children of parents with high ACE loads are at higher risk of carrying significant ACE loads themselves, unless the cycle is interrupted.
Positive Childhood Experiences (PCEs) offer an important message of hope. Unlike ACEs, which identify sources of risk, PCEs help identify sources of resilience.
While Adverse Childhood Experiences (ACEs) increase the risk of mental health difficulties, PCEs are associated with greater resilience, better well-being, and lower risk of mental health problems in adulthood.
One of the most important insights from PCE research is that children do not need perfect childhoods to thrive. Parents and caregivers cannot eliminate every challenge, disappointment, or adversity from a child’s life. However, positive and supportive experiences can have a powerful and lasting impact on development and resilience. (Trivedi et al., 2026)
Research suggests that these experiences can help buffer the effects of adversity and support healthier emotional, psychological, and social outcomes across the lifespan.
This finding also has important implications for parenting. Adults who become aware of their own childhood experiences, recognise unhelpful patterns, learn to regulate their emotions, and work through unresolved adversity often change what their children experience in everyday life. In many ways, the most powerful gift a parent can give a child is their own healing. In doing so, they help create the conditions that foster resilience, emotional well-being, and healthier development in the next generation.
Two books from the Wellness Space team
Much of the research described above is translated for the general reader in two books published by Penguin Random House India. They sit on either side of the same line — one looking back at what happened, one looking forward at what happens next, between an adult and the children they raise.
For the adult exploring their own history — What Happened to Me? vs What’s Wrong with Me?
By Dr Gunjan Y Trivedi, Dr Riri G Trivedi and Dr Hemalatha Ramani (Ebury Press, Penguin Random House India). The book translates ACE research, PCE findings, ACE-14, and Inner Child Therapy into an accessible guide for Indian readers seeking to understand childhood trauma and recovery.
It is also recommended reading for therapists working with Indian clinical populations who want a public-facing reference they can confidently put in a client’s hands.
Available on Amazon India: https://www.amazon.in/What-Happened-Whats-Wrong-Perspectives/dp/9377309352
For parents wanting to break the cycle — This Book Won’t Teach You Parenting
By Dr Riri G Trivedi and Anagha Nagpal (Penguin Random House India). The premise is unusual for the parenting category: this is not a manual of techniques. It is a guided invitation to parents to examine their own inner worlds, their own childhood patterns, their own unhealed wounds, their own self-regulation gaps, so they can raise emotionally healthy children without unconsciously passing on what they did not deal with themselves. Read alongside the PCE research, the book becomes a manual for actively building protective experiences for the next generation.
The book addresses positive parenting in the Indian cultural context, screen time, social media, teen relationships, joint-family dynamics, and offers age-appropriate strategies from toddlerhood to teen years. It includes self-reflection exercises drawn from inner child work and self-regulation techniques drawn from the same evidence base as our clinical practice.
Dr Riri G Trivedi is the co-founder of Wellness Space; her doctoral work is on Adverse Childhood Experiences, anxiety, depression, and subjective well-being in adult Indians, the same body of research that underlies this article. Anagha Nagpal is a certified parent educator and regression therapist.
Available on Amazon India: https://www.amazon.in/This-Book-Wont-Teach-Parenting/dp/0143474103
Both books at a glance
| What Happened to Me? vs What’s Wrong with Me? | This Book Won’t Teach You Parenting | |
Author(s) | Dr Gunjan Y Trivedi, Dr Riri G Trivedi, & Dr Hemalatha Ramani | Dr Riri G Trivedi & Anagha Nagpal |
Publisher | Ebury Press / Penguin Random House India | Penguin Random House India |
Focus | Childhood trauma and ACEs — Indian perspectives | Healing your own childhood wounds while raising children |
| Audience | Adults exploring their own history; therapists | Indian parents at every stage from toddler to teen |
In summary
Childhood trauma is not destiny. Adversity matters, but so do protective experiences. The growing body of Indian research on ACEs, PCEs, resilience, and recovery suggests that understanding our childhood experiences is not about assigning blame; it is about understanding ourselves more clearly, healing what needs healing, and creating healthier futures for the next generation.
If your adult life makes more sense once you map your childhood, the work is not theoretical. It is concrete, measurable, and increasingly evidence-based. Two books from our team, one on the adult journey, one on the parenting journey, can be a starting point. The first step toward clinical work is a structured assessment. The rest follows from there.
For readers interested in going deeper, this article serves as an overview of a larger body of work developed at Wellness Space. The research, clinical models, books, therapy approaches, and practitioner training programmes described throughout this article are all connected by a common goal: helping adults understand the impact of childhood experiences, supporting recovery through evidence-based psychotherapy, and fostering resilience in future generations.
Next steps
If you would like to begin with a structured assessment or 1:1 consultation, you can reach out via our therapy process page or get in touch directly.
If you are a mental health practitioner interested in evidence-based training in trauma-informed psychotherapy, inner child integration, and RTM, see our six-module training programme.
Frequently Asked Questions on childhood trauma, recovery
How do I know if childhood trauma may still be affecting me?
Many adults are unaware that current difficulties may be connected to childhood experiences. Common signs include chronic anxiety, persistent low self-worth, difficulty regulating emotions, recurring relationship patterns, perfectionism, people-pleasing, emotional numbness, and a lingering sense that “something is wrong with me” despite evidence to the contrary. A structured assessment can help clarify whether childhood experiences may be contributing to current difficulties.
I had a difficult childhood, but I function well. Does childhood trauma still matter?
Not necessarily in a negative way. Many people develop remarkable strengths, resilience, and coping skills in response to adversity. However, even highly successful adults may carry hidden burdens such as chronic stress, self-criticism, relationship difficulties, or emotional exhaustion. Understanding childhood experiences is not about finding problems — it is about understanding patterns.
Can childhood trauma be treated?
Yes. Research suggests that many effects of childhood trauma can improve significantly with appropriate support. Evidence-based psychotherapy approaches can help individuals understand the impact of childhood experiences, develop healthier coping strategies, improve emotional regulation, strengthen relationships, and process unresolved trauma. Different people may benefit from different approaches depending on their history, symptoms, and goals.
What is evidence-based psychotherapy?
Evidence-based psychotherapy refers to therapeutic approaches that are informed by scientific research, clinical expertise, and the needs of the individual. In the context of childhood trauma, evidence-based approaches may include trauma-focused therapies, attachment-informed approaches, self-regulation interventions, cognitive and behavioural therapies, and other methods that have demonstrated effectiveness in research and clinical practice.
How can I get help if I think childhood trauma is affecting me?
The first step is usually assessment and understanding. Many people seek support only for symptoms such as anxiety, depression, burnout, relationship difficulties, or low self-esteem without recognising the role childhood experiences may be playing. A trauma-informed assessment can help identify whether childhood adversity, ACEs, or Complex PTSD (CPTSD) may be relevant to your situation and help guide appropriate evidence-based treatment options. You can begin by clicking here.
What can parents do to break the intergenerational cycle?
Parents do not need to be perfect. One of the most powerful steps is becoming aware of their own childhood experiences and how those experiences may influence parenting. Adults who learn to regulate their emotions, process unresolved adversity, and develop healthier relationship patterns often change what their children experience in everyday life, helping to build resilience in the next generation.
What should mental health practitioners know about ACEs, PCEs, and CPTSD?
The growing research literature suggests that childhood adversity and protective experiences both play important roles in adult mental health. Practitioners may benefit from training in trauma-informed care, evidence-based psychotherapy, Complex PTSD, attachment, self-regulation, and developmental trauma. Understanding both ACEs and PCEs can help create a more balanced formulation that recognises risk factors as well as sources of resilience.
Where can mental health practitioners learn more?
Practitioners interested in childhood trauma, ACEs, PCEs, Complex PTSD (CPTSD), Inner Child Therapy, RTM, and evidence-based psychotherapy may find value in the research, clinical resources, books, and training opportunities developed by the Wellness Space team.
A useful starting point is the six-module Evidence-Based Psychotherapy Training Programme, which introduces participants to trauma-informed assessment, ACEs and PCEs, Inner Child Therapy, Complex PTSD, self-regulation, and Reconsolidation of Traumatic Memories (RTM), alongside the research evidence supporting these approaches in Indian populations.
Which book should I start with?
If you are exploring your own childhood experiences and their impact on adult life, What Happened to Me? vs What’s Wrong with Me?: Indian Perspectives on Childhood Trauma and Recovery is the best starting point. If you are a parent seeking to create healthier experiences for your children and avoid repeating old patterns, This Book Won’t Teach You Parenting may be more relevant.
Is childhood trauma destiny?
No. Childhood adversity increases risk, but it does not determine the future. Research on Positive Childhood Experiences (PCEs), resilience, and recovery consistently shows that supportive relationships, emotional safety, self-awareness, and evidence-based psychotherapy can help people build healthier and more fulfilling lives.
References
- Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., Edwards, V., Koss, M. P., & Marks, J. S. (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study. American journal of preventive medicine, 14(4), 245–258. https://doi.org/10.1016/s0749-3797(98)00017-8
- Huynh, P. A., Kindred, R., Perrins, K., de Boer, K., Miles, S., Bates, G., & Nedeljkovic, M. (2025). Prevalence of Complex Post-Traumatic Stress Disorder (CPTSD): A Systematic Review and Meta-Analysis. Psychiatry Research, 351, 116586. https://doi.org/10.1016/j.psychres.2025.116586
- Trivedi, G. Y., Pandya, N., Thakore, P., Ramani, H., Trivedi, R. G., & Kathirvel, S. (2024). The effectiveness of Reconsolidation of Traumatic Memories for Complex PTSD – A pilot quasi-experimental study from a wellness centre in India. European Journal of Trauma & Dissociation, 8(4), 100480. https://doi.org/10.1016/j.ejtd.2024.100480
- Trivedi, G. Y., Pillai, N., & Trivedi, R. G. (2021). Adverse Childhood Experiences & mental health – the urgent need for public health intervention in India. Journal of preventive medicine and hygiene, 62(3), E728–E735. https://doi.org/10.15167/2421-4248/jpmh2021.62.3.1785
- Trivedi, G. Y., Surana, P., Pandya, N., Patel, N., Trivedi, R. G., Kathirvel, S., & Kumar, A. (2025). Psychometric properties of expanded adverse childhood experiences assessment questionnaire at a wellness centre in India. Asian journal of psychiatry, 108, 104523. https://doi.org/10.1016/j.ajp.2025.104523
- Trivedi, R. G., Kumar, A., Soundappan, K., Trivedi, G. Y., Ramani, H., & Kumar, S. (2025). Association between Adverse Childhood Experiences and Internalizing Symptoms in Adults at a Wellness Centre in India. Indian journal of community medicine : official publication of Indian Association of Preventive & Social Medicine, 50(3), 472–478. https://doi.org/10.4103/ijcm.ijcm_419_23
- Trivedi, G. Y. (2026). Positive childhood experiences are independently associated with adult resilience after accounting for adverse childhood experiences: A cross-sectional study in India. Acta Psychologica, 267, 107028. https://doi.org/10.1016/j.actpsy.2026.107028

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Leave A Comment