
Trivedi Depression Pathways™: A Trauma-Informed Model for Recurring Depression
Depression isn’t one illness. It’s many doorways into the same room — and each one needs a different key.
Why “just depression” is rarely just depression
For decades, depression has been talked about as one thing — usually framed as a chemical imbalance, usually treated with one class of medication. That framing has helped many people. But it has also left many others wondering why the standard approach hasn’t been enough, or why their depression keeps returning even after “successful” treatment.
Part of the reason is that depression rarely arrives alone. It shows up inside many other diagnoses:
- In Major Depressive Disorder (MDD), it is the primary picture.
- In Borderline Personality Disorder (BPD), depressive episodes are often interwoven with emotional dysregulation and relational pain.
- In Post-Traumatic Stress Disorder (PTSD), low mood, numbness, and hopelessness are common companions to the more visible symptoms.
- In Complex PTSD (CPTSD), persistent depression, shame, and a damaged sense of self are often the dominant features — sometimes more so than the trauma flashbacks themselves.
This is why two people with the same diagnostic label can have very different inner experiences, very different histories, and very different recovery needs.
The pathways depression can travel
In our clinical and research work at Wellness Space, several pathways (Figure 1) into depression appear again and again. Most people who carry depression have travelled more than one:
- Childhood adversity that was never fully processed
- Emotional neglect — the slow erosion of being unseen, unheard, or unsoothed
- Loneliness and weak social support that compound over years
- Low resilience built up by repeated overwhelm
- Chronic anxiety and insomnia are wearing the system down
- Nervous-system exhaustion — the body’s regulation system running on empty
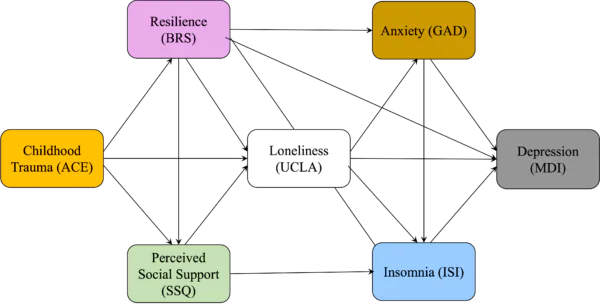
Figure 1 – Key Building blocks of Trivedi Depression Pathways™
Knowing which pathways are active and in what proportion makes recovery work targeted rather than generic. The full mapping — and how each pathway is identified and addressed — is detailed in our book What Happened to Me?
Why this matters for recovery
When depression is treated as a single thing, the response is necessarily generic. When the underlying pathways are mapped, treatment can be shaped to the actual roots — sometimes medication, often psychotherapy, frequently body-based and nervous-system work, occasionally relational and family-system work, and almost always more than one of these in combination.
The Trivedi Depression Pathways™ model is intended to help both individuals and practitioners identify the deeper emotional and developmental roots of depressive symptoms — and then act on them. It works alongside other Wellness Space frameworks, including the Pancha Kosha Trauma Framework™, the PsyComplexity Scale™, and the Trivedi FLIP Model™.
Who this is for
- Adults with persistent or recurring depression who sense that something more than brain chemistry is at work
- People in long-term treatment are looking for a more complete formulation of their experience
- Family members trying to understand what a loved one is actually living with
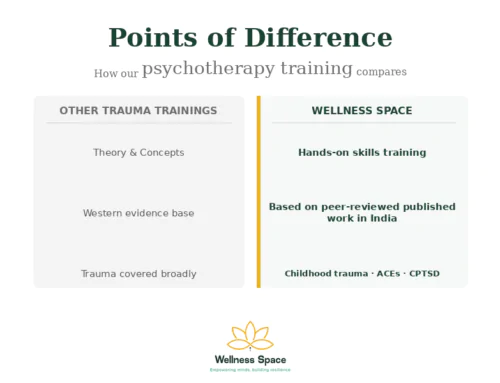
- Therapists and clinicians seeking a trauma-informed framework that goes beyond symptom checklists
Frequently asked questions
Q. Are you saying depression isn’t biological? No. Biology is real and matters. What we are saying is that depression is rarely only biological. The Trivedi Depression Pathways™ treats biology as one strand within a wider system that also includes history, conditioning, relationships, and nervous-system regulation.
Q. My diagnosis is BPD/PTSD/CPTSD, not depression. Does this framework still apply? Yes. Depression is woven into many trauma-related diagnoses, even when it isn’t the headline label. The pathways framework can help identify which roots are driving the depressive features within your broader picture. The book walks through this in detail.
Q. Should I stop my medication? Please do not stop or change psychiatric medication based on a website or a therapist’s guidance. Medication decisions are made with your prescribing doctor (psychiatrist). The framework complements medical care — it does not replace it. Many of our clients are on medication while also doing this deeper work.
Q. If I have a high ACE score, am I destined to get depression? No. Adverse childhood experiences raise risk; they do not determine outcome. Many people with significant childhood adversity never develop depression, and many who do recover fully. The role of social support, positive childhood experiences (PCEs), etc play a balancing role.
Q. Is this appropriate if I’m in crisis right now? If you are in crisis or thinking about harming yourself, please reach out for immediate support — speak to someone you trust and contact a local mental health helpline or emergency service (in India:1-800 891 4416). The pathways framework is most useful as part of ongoing, stable therapeutic work, not as a substitute for crisis care.
Learn the full pathways model
The Trivedi Depression Pathways™ — including the diagnostic mapping, the clinical pathways in detail, and the case narratives — is detailed in our book What Happened to Me?

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Leave A Comment