
The role of emotions in obesity.
Obesity in India has reached epidemic proportions in the 21st century, with morbid obesity affecting a significant portion of the country’s population. That overweight and obesity prevalence will increase to 30% and 9.5% among men and 28 and 14% among women by 2040[1].
Despite increased health awareness of more physical activities, obesity continues to grow! This trend needs investigation. In our coaching and therapeutic practice at Wellness Space, we get many clients who say that despite dieting, gymming, yoga and other workouts, they still don’t seem to lose weight. Others admit that they cannot sustain the diet or exercise or tend to have bouts of binging – which takes them back to square one! This is where we need to ask the essential question about the role of emotions in obesity.
Is there a role of emotion in obesity?
The research confirms a significant correlation between negative emotional states with binge eating or eating disorders[2] [3]. Poor emotional regulation skills and depression are proven to be the cause of Obesity and its result! All this indicates one area where there is a complete lack of focus regarding obesity – and that is the role of emotions! Often food becomes a respite from stress, loneliness or emptiness. Sadness and Depression result in the clients going into compulsive eating sprees. This sadness and depression are also usually connected to life events, and once these are healing through therapy, the compulsive eating reduces or stops.
Emotional Trauma in childhood has a massive correlation with obesity among those adults. Research shows that there is a significantly higher correlation between sexual abuse and victimisation in childhood with Extreme obesity among women (Figure 1)[4] [5]. However, the current mode of interventions across the industry hardly consider the role of emotions (i.e. mind) in obesity!
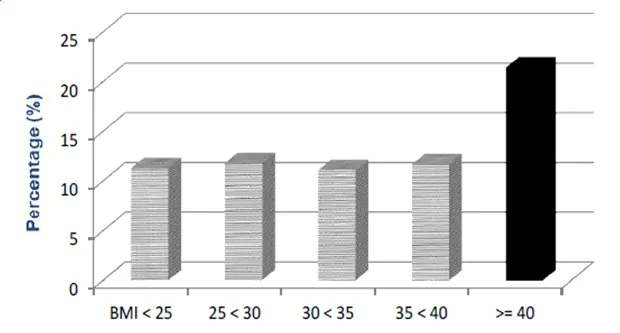
Figure 1 – Source[5]. The graphic shows that individuals who experience multiple childhood maltreatment (rape, molestation, physical assault) shown by the dark black bar are more likely to be dangerously obese, as denoted by BMI numbers.
Scientific evidence on emotions and obesity:
- The role of emotions (i.e. mind) in driving energy imbalance of energy (in the body) is critical and demonstrated by scientific research[6] [7]. There is clear evidence confirming the role of negative emotions and poor emotion regulation strategies in the onset and maintenance of binge eating in Binge Eating Disorder(BED) and loss of control in eating[8] [9].
- There is an association of emotional eating with depression and poor emotional regulation skills, indicating that obese individuals with high emotional eating must not focus only on a calorie-restricted diet but must also work on emotional regulation skills[10].
- A study of 3000 candidates for bariatric surgery (a stomach procedure to reduce obesity) also validated the history of persistent negative emotions. The study found that BMI was very high if the subject had experienced both childhood abuse and PTSD (Post Traumatic Stress Disorder). The presence of both negative experiences (and their impact on negative emotions) resulted in more severe physical and physiological morbidity than those who experienced abuse alone[11]!
- Research has also identified a very high prevalence of obesity (almost twice) in adolescents for individuals who had poor relationships with their mothers compared to those who had good relationships. Again, a validation that extreme or sustained stress responses are associated with dysregulation of body systems involved in energy balance, leading to obesity, and the intervention must include emotional regulation[12].
- A strong inverse relationship between mood disorder and obesity[13], and a comprehensive review of the evidence in this area identified a circle of discontent as the critical driver of homeostatic imbalance identifying weight gain with negative affect, body dissatisfaction and over-consumption[14].
- Sleep disruption is associated with an increase in ghrelin and a decrease in leptin hormone, which increases the risk of hunger and appetite. Moreover, obesity is also linked to sleep disorders and hence the need to review and address sleep quality issues for managing obesity[15].
Together, the above insights demonstrate the role of negative emotions in obesity and highlight the importance of addressing chronic negative emotions since suppressed emotions contribute significantly to emotional health, further increasing the risk of obesity.
The mind and body balance and obesity
To summarise the real problem, obesity is an imbalance of both the mind and the body. Let’s consider the more specific aspect first. Everyone understands that the imbalance in energy through higher calorie intake and lower-calorie burning adds more fat to the body. The contributors of this body imbalance or energy imbalance include lifestyle choices such as (a) limited physical activity, (b) poor quality, calorie-rich food and a combination of other factors. As discussed earlier, most of the work in managing weight (or obesity) focuses on restoring the energy balance in the body. Unfortunately, the research now has demonstrated that it is not sufficient to just work on the energy balance in the body. The role of the mind, emotions are well established. Specifically, imbalance in emotions, i.e. more negative emotions caused by life events, body dissatisfaction, etc., plays an important role. If these conditions persist, the emotional imbalance contributes towards the body imbalance[16].
How to address the emotional balance!
It is possible to address the negative emotions that we carry on a regular basis. Therapies like Regression therapy and Inner Child Integration therapy have techniques (The Release Reframe Toolkit) to help clients release the physical and emotional blockages resulting from childhood abuse or trauma.
Therapeutic intervention helps release the emotional charge (or implicit emotions), and then the mind and body are more conducive to self-regulation processes.
Individual therapeutic intervention with Wellness Space
Several of our insights and research confirm that it is possible to reduce negative emotions. We study the emotional footprint of the individual through several psychological assessments (WHO-5 Wellbeing Index, MDI-Major Depression Inventory, GAD-Generalized Anxiety Disorder, Specific Phobia, Sleep Quality – through Insomnia Severity Index) so that together with the client, the coach can identify the gap and address it. Few examples are captured below:
- Figure 2 shows the data of 91 individuals who completed four sessions of Regression Therapy & Life coaching. These individuals’ depression levels reduced from very high to “none” and their anxiety level went down to “acceptable” levels!
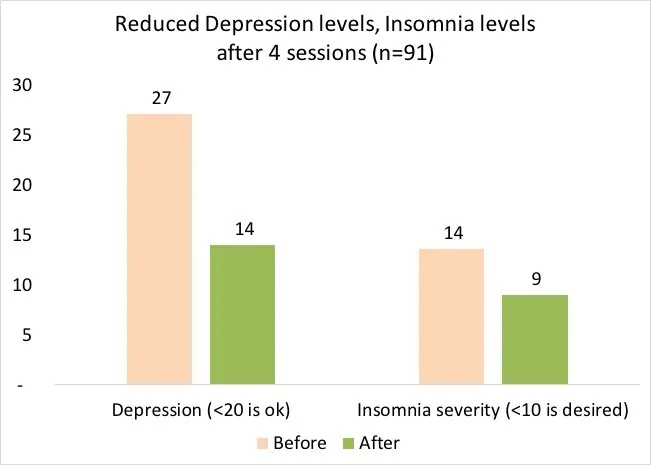
Figure 2: Statistically significant improvement in mood (shown by reduction in anxiety and depression levels, n=91, after just 4 sessions)
- Figure 3 shows how, after eight Regression Therapy & Life Coaching sessions, the individuals’ show a significant reduction in anxiety and depression. At the same time, their well-being and sleep quality increase!
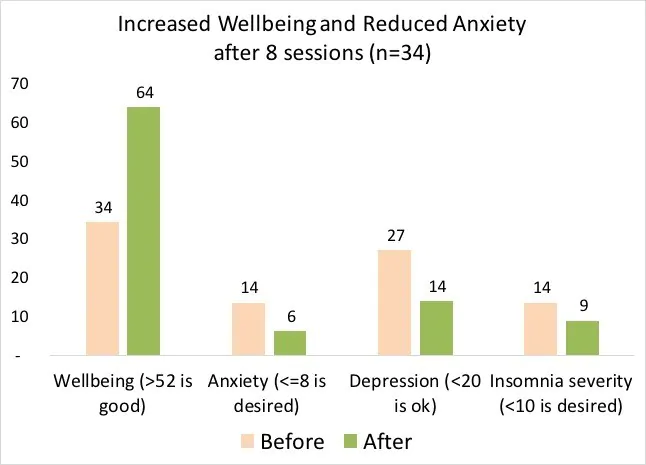
Figure 3: Overall trend after eight sessions (n=34)
Self-regulation using the SEE Protocol for Self Hypnosis:
Our research in active meditation through the SEE Protocol of Self-hypnosis demonstrates a significant decrease in negative mood and an increase in a positive mood and changes in the body as measured by heart rate variability. Thus, regular practice of self-hypnosis can help in enhancing the mood, increase sleep quality, and reduce overall negative emotions.
Please read about the SEE Protocol research here. If you wish to learn the SEE Protocol, you can join the “Journey Within” workshop (12 hours, online).
To summarize, there is sufficient scientific evidence on the role of emotions in Obesity. By recognizing this mind-body connection and the need for emotional balance, we become open to creating an obesity management plan that includes balancing the emotions and enhancing the quality of life while working on the physical body related energy balance!
Gunjan Y Trivedi
Contact +91-9099853844
References:
[1] Luhar, S., Timæus, I. M., Jones, R., Cunningham, S., Patel, S. A., Kinra, S., Clarke, L., & Houben, R. (2020). Forecasting the prevalence of overweight and obesity in India to 2040. PloS one, 15(2), e0229438. https://doi.org/10.1371/journal.pone.0229438
[2] Görlach, M. G., Kohlmann, S., Shedden‐Mora, M., Rief, W., & Westermann, S. (2016). Expressive suppression of emotions and overeating in individuals with overweight and obesity. European Eating Disorders Review, 24(5), 377-382.
[3] Levitan, R. D., & Davis, C. (2010). Emotions and eating behaviour: Implications for the current obesity epidemic. University of Toronto Quarterly, 79(2), 783-799.
[4] Luppino FS, de Wit LM, Bouvy PF, et al. Overweight, Obesity, and Depression: A Systematic Review and Meta-analysis of Longitudinal Studies. Arch Gen Psychiatry. 2010;67(3):220–229. doi:10.1001/archgenpsychiatry.2010.2
[5] Timothy DB,Patrick MO,Bonnie SD,Kilpatrick DG (2016) Extreme Obesity and its Associations with Victimization, PTSD, Major Depression and Eating Disorders in a National Sample of Women: The Controlled Overeat. J Obes Eat Disord 1:10. doi: 10.4172/2471-8203.100010
[6] American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. American Psychiatric Publishing; Arlington, VA, USA: 2013
[7] Clyne, C., & Blampied, N. M. (2004). Training in Emotion Regulation as a Treatment for Binge Eating: A Preliminary Study. Behaviour Change, 21(04), 269–281. doi:10.1375/bech.21.4.269.66105
[8] Dingemans, A., Danner, U., & Parks, M. (2017). Emotion Regulation in Binge Eating Disorder: A Review. Nutrients, 9(11), 1274. doi:10.3390/nu9111274
[9] Goldschmidt, A. B., Lavender, J. M., Hipwell, A. E., Stepp, S. D., & Keenan, K. (2017). Emotion Regulation and Loss of Control Eating in Community-Based Adolescents. Journal of abnormal child psychology, 45(1), 183-191.
[10] van Strien T. (2018). Causes of Emotional Eating and Matched Treatment of Obesity. Current diabetes reports, 18(6), 35. doi:10.1007/s11892-018-1000-x
[11] Walsh, E., Rosenstein, L., Dalrymple, K. et al. The Importance of Assessing for Childhood Abuse and Lifetime PTSD in Bariatric Surgery Candidates, J Clin Psychol Med Settings (2017) 24: 341. https://doi.org/10.1007/s10880-017-9518-7
[12] Anderson, S. E., Gooze, R. A., Lemeshow, S., & Whitaker, R. C. (2012). Quality of early maternal-child relationship and risk of adolescent obesity. Paediatrics, 129(1), 132-40.
[13] Singh M. (2014). Mood, food, and obesity. Frontiers in psychology, 5, 925. doi:10.3389/fpsyg.2014.00925
[14] Marks, D. F. (2015). Homeostatic theory of obesity. Health Psychology Open. https://doi.org/10.1177/2055102915590692
[15] Trivedi, G. T., Saboo, B., & Hasnani, D. (2018). Importance of screening for sleep disorders (Chronic disease). J Clin Diabetol, 5, 3.
[16] Marks, D. F. (2015). Homeostatic theory of obesity. Health Psychology Open. https://doi.org/10.1177/2055102915590692

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Leave A Comment